Главная страница Случайная страница
КАТЕГОРИИ:
АвтомобилиАстрономияБиологияГеографияДом и садДругие языкиДругоеИнформатикаИсторияКультураЛитератураЛогикаМатематикаМедицинаМеталлургияМеханикаОбразованиеОхрана трудаПедагогикаПолитикаПравоПсихологияРелигияРиторикаСоциологияСпортСтроительствоТехнологияТуризмФизикаФилософияФинансыХимияЧерчениеЭкологияЭкономикаЭлектроника
Methods of Examination. Complaints. The endocrine system has multiple effects on various bodily functions and the patient's complaints are therefore varied
|
|
Inquiry
Complaints. The endocrine system has multiple effects on various bodily functions and the patient's complaints are therefore varied. The patient may complain of increased excitability, interrupted and superficial sleep, impaired memory, irritability, hyperhidrosis, chills, heart palpitation, noise in the ears, blood rush to the head, skin itching, increased thirst, and considerable wasting. When inquiring the patient, the physician can reveal some features of his nervous and psychic character that may suggest some endocrine diseases: e.g., fussiness, rapid movements, hasty speech, apathy, and flaccidity suggest thyroid dysfunction, while mental underdevelop-ment, and its degree—infantilism and cretinism.
Anamnesis. It is important to establish the direct cause of the disease. Strong emotions, fear, and psychic traumas are the predisposing factors for thyrotoxic goitre. Endocrine diseases often develop during sexual maturation, after childbirth, and during menopause.
The hereditary factor is also important in endocrine diseases, e.g. in diabetes mellitus. The endocrine function can be affected by some other diseases. Tuberculosis of the adrenal glands, for example, is the cause of their hypofunction (Addison's disease).
Physical Examination
INSPECTION
Inspection of the patient is a valuable diagnostic procedure. Sometimes the diagnosis becomes clear at first sight. The patient's appearance and some special features of his behaviour are quite characteristic in diffuse thyrotoxic goitre, myxoedema, acromegaly, nanism (dwarfism), pituitary cachexia, Itsenko-Cushing syndrome, Addison's disease, upset fat metabolism, etc.
Endocrine diseases, especially affections of the thyroid and pituitary glands, can alter the expression of the patient's face. Patients with thyroid hyperfunction have large, wide open, protruded eyes; winkling is rare, the eyes are lustrous, and the patient's face has the expression of horror or fear. The face of patients with thyroid hypofunction (myxoedema) is
38-1556
Special Part
Chapter 10. Endocrine System and Metabolism
 round, without wrinkles, with motionless eyes; the general expression is dullness and apathy. The acromegalic face is characterized by protruding superciliary arches, abnormally large nose, lips, tongue and the chin; the abnormally large lower jaw has widely set teeth (diastema). Pituitary hypofunction is attended by obesity which gives the woman-like expression to the male face.
round, without wrinkles, with motionless eyes; the general expression is dullness and apathy. The acromegalic face is characterized by protruding superciliary arches, abnormally large nose, lips, tongue and the chin; the abnormally large lower jaw has widely set teeth (diastema). Pituitary hypofunction is attended by obesity which gives the woman-like expression to the male face.
Neck. Inspection of the anterior surface of the neck can reveal the size of the thyroid gland (its enlargement).
Height. Gigantism (over 195 cm) is mostly the result of anterior pituitary hyperfunction (acromegalic gigantism) or hypofunction of the sex glands (hypogonadal gigantism). Dwarf ism (the height below 135 cm) can be due to hypofunction of the anterior pituitary lobe with preservation of childish proportions of the body, underdevelopment of the sex organs, and the absence of the secondary sex characters. The same symptoms can be observed in marked thyroid hypofunction with signs of myxoedema and mental retardation (to idiotism).
Skin. Pallid face with a yellowish hue is characteristic of myxoedema; the face is hyperaemic in Itsenko-Cushing syndrome (anterior pituitary hyperfunction); the mucosa and skin are bronze (especially skin folds, the palms) in patients with Addison's disease (adrenal hypofunction). Dry and scaling skin is characteristic of thyroid and parathyroid hypofunction; the skin is dry and cold in hypothyroidism. The skin is smooth and moist in patients with hyperthyroidism. Thickening of the skin associated with hypertrophy of its papillar layer is found in acromegaly. Oedema of the skin which is characteristic of hypothyroidism is due to its impregnation with mucinous substance. The Itsenko-Cushing syndrome is characterized by atrophy of the skin on the femur and the abdomen (red-violet striae). Scratching of the skin and furunculosis, cholesterol deposition in the skin of the eyelids is often observed in diabetes mellitus. Nails are brittle in hypothyroidism and tetany.
Hair. Changes in hair is an important diagnostic sign in endocrine diseases. A female pattern of hair growth in men is typical of eunuchoidism, while male-type pilosis in women occurs in acromegaly and Itsenko-Cushing syndrome; falling of hair from the eyelids, brows, mustaches, and the head is characteristic of myxoedema.
Subcutaneous fat. Uniform distribution of fat over the entire body is characteristic of thyrogenic obesity, while deposition of fat mostly in the pelvic region (lower abdomen, buttocks, thighs) occurs in pituitary and pubertal obesity. Excess fat on the face and trunk is a sign of the Itsenko-Cushing syndrome. Excess wasting is observed in some forms of diabetes mellitus and thyrotoxic goitre. Cachexia is a sign of Simmonds's disease which is due to the affection of the pituitary gland (pituitary cachexia).
Bones. Eunuchoidism is characterized by a delayed growth of the epiphyseal ends of long tubular bones. Acromegaly is marked by abnormal thickening of the enlarged bones of the skeleton.
Muscles. The hormone of the parathyroid glands is produced in deficient quantity and the blood calcium content is thus decreased. As a result, patients develop tonic convulsions (mostly of the flexor muscles). The patient's hand is flexed to give the specific appearance of the " obstetrician hand". When the facial muscles are affected by convulsions, the face acquires the expression of a forced smile. The muscles are developed in excess in acromegaly.
The thyroid and the testes are the only endocrine glands that are ac
cessible to direct inspection...-...,
PALPATION
The thyroid gland is studied by palpation. Tentative palpation assesses the density of the organ, the character of its surface, and the presence of nodes. Then follows special palpation. The examiner places four flexed fingers of both hands deep beyond the posterior edges of the ster-nocleidomastoid muscle, and the thumbs beyond the anterior edges of this muscle. The patient is now asked to make swallowing movements: the thyroid together with the larynx moves between the examiner's thumbs. This method is used to reveal even insignificant enlargement of the thyroid gland that cannot be detected by common palpation. Mobility of the gland during swallowing, the presence or absence of pulsation, and tenderness of the thyroid can also be determined by this method. Palpation of one lateral lobe of the gland can be facilitated by pressing the thyroid cartilage on the opposite side. The thyroid isthmus is palpated by the sliding movements of the examining fingers in the direction of the sternal manubrium. The lower portion of the thyroid, which is concealed behind the sternal manubrium, may be affected by nodes. In order to palpate them (for outlining their borders and assessing their consistency), the patient is asked to make swallowing movements, while the examiner's fingers palpate the thyroid in the suprasternal notch.
In order to follow up changes in the size of the thyroid gland, it is important to determine its size. The girth of the neck, the transverse dimension of the thyroid and the size of its separate nodes should be determined. When measuring the girth of the neck, one end of the measuring tape should be fixed on the crest of the 7th cervical vertebra, the tape being passed over the most prominent part of the thyroid. When taking transverse measurements, the tape is placed beyond the outer posterior edges of the sternocleidomastoid muscles and passed over the anterior sur-
38*
Special Part
Chapter 10. Endocrine System and Metabolism


 face of the thyroid gland. The diameter of separate lymph nodes of the thyroid gland is determined by bow compasses with rounded ends.
face of the thyroid gland. The diameter of separate lymph nodes of the thyroid gland is determined by bow compasses with rounded ends.
Palpation gives a more detailed information on the structure of the skeleton and the condition of the skin of patients with endocrine diseases that were first revealed by visual examination.
Percussion can reveal a retrosternal struma (goitre).
AUSCULTATION
Sounds and murmurs can be heard over the enlarged thyroid in patients with thyrotoxicosis. These are explained by accelerated flow of blood and its intensified supply to the thyroid gland.
Laboratory studies
Determination of protein-bound iodine (PBI) in the blood serum is widely used to study the thyroid function because 90—95 per cent of protein-bound iodine is the iodine of thyroxin. The level of the protein-bound iodine in healthy adults varies from 315 to 630 nmol/1 (4-8 mg/100 ml). Figures below 275 nmol/1 (3.5 mg/100 ml) indicate hypothyroidism, and above 670 nmol/1 (8.5 mg/100 ml) hyperthyroidism. If high PBI persists for a year and does not vary with increasing content of thyroid hormones in the blood, it may be due to administration of contrast iodine-containing substances (for X-ray examination) and iodine therapy (saiodin, enteroseptol, mexase, etc.). The blood serum of patients with parathyroid hypofunction is examined for calcium and phosphorus; the content of these elements decreases in tetany.
Aldosterone and hydroxycorticosteroids are found in decreased quantity in patients with diseases of the adrenal glands (Addison's disease); the content of potassium and sodium salts increases in these patients. In suspected diabetes mellitus (and also in the presence of this disease) the blood and urine are tested for sugar (see below).
DETERMINING BASAL METABOLISM
| RQ = |
Basal metabolism is the amount of energy produced by the body at rest which is only necessary to maintain the vitally important processes, such as respiration, circulation of blood, body temperature, the function of the kidneys, etc. The produced energy is the result of oxidation of proteins, fats, and carbohydrates taken with food with the corresponding consumption of oxygen. Once the amount of oxygen consumed by the body is known, the released energy (in calories) can be determined by multiplying the amount of oxygen by its heat equivalent. The heat equivalent of oxygen is different for combustion of proteins, fats, and carbohydrates. It has been found that it agrees with the respiratory quotient (RQ): CO2 volume produced in respiration
 O2 volume consumed
O2 volume consumed
Therefore, RQ is calculated in addition to the determination of consumption of O2 and production of CO2.
Basal metabolism is determined in the morning before the breakfast. The patient is in the lying position, at complete rest, in a warm and silent room. After the patient has adapted to the conditions of the experiment the gas exchange is studied for 5—10 minutes.
There are two systems (open and closed) for the determination of gas exchange. With the open system, the patient breathes with atmospheric air while the expired air is collected in a closed reservoir where O2 and CO2 are determined and RQ is then calculated. Oxygen breathing is used in the closed system. The patient's nose is clamped and a mouth-piece is introduced into his mouth. The mouth-piece is provided with the inlet and outlet valves; it is connected with a spirometer containing oxygen and provided with a CO2 absorber. During inspiration, oxygen passes into the lungs and the expired air is returned to the spirometer. The decrease in the initial volume of oxygen is recorded automatically on a moving chart. The amount of carbon dioxide is not determined by this method, and a protein-free diet should therefore be given to the patient, three days before the examination. In this case RQ nears 0.8. This quotient is adopted conventionally as a constant for calculations. Automatic recording instruments of the closed type (metabolimeters) are much simpler and therefore widely used in practical medicine. Oxygen consumption during 5 or 10 minutes of the experiment is recalculated for 24 hours with reference to the calorific value of oxygen, atmospheric pressure, and the ambient temperature (the latter two factors are important for the volume of gas).
The results of the determination of basal metabolism are assessed by comparing the findings with the amount of energy that a healthy individual of the same body-build spends in conditions of basal metabolism. Basal metabolism depends on the weight of an individual, his height, age, and sex. The reference values can be found in standard tables. In a healthy individual the findings are usually close to the reference (tabulated) ones and only differ by not more than ±15 per cent.
Basal metabolism in patients with pronounced thyrotoxicosis usually increases by 30—100 per cent and in patients with myxoedema it decreases by 20—30 per cent and more. But basal metabolism depends also on some other pathological conditions. It increases in diabetes mellitus, fever of any aetiology, leucosis, polyglobulia; it decreases in anaemia, especially in pernicious anaemia, and in Addison's disease. Increased oxygen demands in patients with heart failure do not indicate increased basal metabolism but oxygen deficiency.
RADIOISOTOPE STUDIES
Absorption of 131I by the thyroid gland. Accumulation of radioactive iodine in the thyroid gland during 2-24 hours is determined either by a contact method using the Geiger-Mueller counter, or by scintillation instruments (at a distance of 10-30 cm). Remote measurements are more accurate because they do not depend on thickness of the tissues overlying the thyroid gland, its configuration, or structure. A flCY-60 unit is used in the Soviet Union for the purpose. It can be used not only to diagnose thyroid dysfunction but also to locate tentatively the tumour metastases and the degree of accumulation of 131I in the right and left lobes of the thyroid gland.
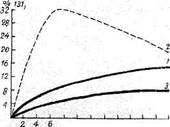
Normal accumulation of 131I in the thyroid gland during two hours is 7-12 per cent, and during 24 hours 20-29 per cent. In patients with thyrotoxicosis, these figures are 9.5-72 and 11-89 per cent, respectively,
Special Part
Chapter 10. Endocrine System and Metabolism
 | |||||
 | |||||
 | |||||
| 8 to tZ 14 W 18 ZO 22 24 hours |
Fig. 110. Accumulation of iodine in the thyroid gland. 1 —in norm; 2 —in thyrotox-icosis; 5—in hypothyroidism.
while in patients with myxoedema 1-2 and 1-2 per cent, respectively. A more reliable test for thyrotoxicosis is the determination of the rate of absorption and removal of 131I by the thyroid gland. The 131I content in the thyroid gland is determined in 2, 4, 6, 8, and 24 hours following its administration. The follow-up studies of radioactive iodine accumulation in the thyroid gland can be shown graphically where the thyroid function is described by a curve (Fig. 110).
Excretion of mI in the urine. This is another valuable method of evaluating the thyroid function. Healthy individuals excrete 31-63 per cent of radioactive iodine in the urine during the first 24 hours, while patients with thyrotoxicosis excrete 3-22.5 per cent and with hypothyroidism 36—71 per cent.
| -; < < *• |
 Scanning. This technique is used to determine the shape, size, location, and functional condition of the thyroid gland. Scanning is also used to reveal hyperfunctioning " warm" and " cold" nodes in the thyroid tissue, and to determine metastases of tumours (Fig. 111).
Scanning. This technique is used to determine the shape, size, location, and functional condition of the thyroid gland. Scanning is also used to reveal hyperfunctioning " warm" and " cold" nodes in the thyroid tissue, and to determine metastases of tumours (Fig. 111).

Fig. 111. Scanogram of a normal thyroid.
X-RAY STUDY
X-rays are used to detect bone thickening and the enlarged sella turcica in patients with acromegaly. These are indirect evidence of pituitary affection (usually by tumour). Angiograms and retropneumoperitoneum reveal tumours of the adrenal glands; radiographs can reveal retrosternal goitre, deposition of calcium in the thyroid, and displacement and compression of the trachea and oesophagus by the thyroid gland.
THERMOGRAPHY
Thermography is the method of recording infra-red radiation by an instrument sensitive to heat. Intense local infra-red radiation can be detected on a thermogram during the study of patients with thyroid cancer. It is recommended to combine thermography with scanning for diagnosis of tumours of the thyroid gland.