Главная страница Случайная страница
КАТЕГОРИИ:
АвтомобилиАстрономияБиологияГеографияДом и садДругие языкиДругоеИнформатикаИсторияКультураЛитератураЛогикаМатематикаМедицинаМеталлургияМеханикаОбразованиеОхрана трудаПедагогикаПолитикаПравоПсихологияРелигияРиторикаСоциологияСпортСтроительствоТехнологияТуризмФизикаФилософияФинансыХимияЧерчениеЭкологияЭкономикаЭлектроника
Developments in Laboratory Diagnosis
|
|
Improvement of methods to diagnose internal diseases is related to the advances in science and technology. Wide-scale application of new diagnostic techniques in various branches of medicine helps in making the most accurate diagnosis. Highly informative laboratory and instrumental methodologies are currently being used at large research medical centres and major clinics and hospitals.
Application of computers has radically broadened the possibilities of the existing medical equipment and promotes automation of many processes such as control, recovery, and storage of the necessary diagnostic information in computers. This enables simultaneous recording and processing of various parameters of the body organs and systems performance to reveal the presence (or alternately the absence) of a syndrome, and also provides models of body functioning in various conditions, critical ones included.
Microprocessors may be used for automated history taking in several patients simultaneously. The patient has only to answer questions that are displayed on the TV screen by pressing an appropriate button on the keyboard. Depending on the answer, the microprocessor presents new questions that verify and detail the collected data. Such apparatus have become an invaluable diagnostic aid in routine medical examinations of the population. Computers help automate many labour-taking processes in laboratory diagnosis (e.g. counting blood cells, their distribution by size, determining motility of various microorganisms) which is especially important in rapid diagnosis. Data banks that are to contain exhaustive information on each patient are being established in the clinic, each physician and researcher having a personal computer at hand. Using computers on a wide scale would, in many respests, change our current concepts of physicians' labour and the peculiarities of the diagnostic process.
Instrumental diagnostic techniques are being constantly improved. New methods of X-ray studies are actively incorporated into everyday medical practice. These techniques include large-frame photofluorography, angio-graphy, etc. The accuracy and reliability of radionuclide diagnostic techniques have been substantially improved and new gamma-chambers have been developed. Computed tomography (CT) has become a routine technique to visualize the internal structure of organs with rapid and precise mathematical processing of the obtained findings. This technique can, for example, reveal minutest tumorous lesions in the internal organs, and thus is of great diagnostic value. Nuclear magnetic resonance (NMR) is now being effectively used for the diagnosis of various diseases. This is a tech-
41-1556
Appendix
Developments in Laboratory Diagnosis
nique for sectional imaging of the body based on the chemical analysis (absorption of specific radio frequencies by atomic nuclei).
Ultrasonography has also become a very important diagnostic modality. One- and two-dimensional echography, and also Doppler sonography reveal some lesions of the internal organs (eg. tumours) and structures that fail to be detected radiologically.
Endoscopic examination is another diagnostic modality that undergoes further improvement. This technique is used to visualize the internal organs under natural illumination. Combined use of various diagnostic methods (e.g. endoscopy under echographic control, endoscopy with subsequent administration of contrast medium and X-ray examination) is being introduced on a wider scale. Thermography and thermovision have also been widely used for detection of pathological processes (e.g. inflammation) in various organs by variation of temperature in definite areas of the patient's body.
Biopsy sampling of various internal organs is being used more intensively. A new branch of medicine has developed—clinical morphology. Its main object is the clinical, rather than the pathologico-anatomic diagnosis aimed at timely detection of the disease, determination of its characteristic features, and choosing of optimal therapy.
Clinical immunology, genetic engineering, and medical genetics have become of major importance in the diagnosis of internal diseases. Current techniques of laboratory diagnosis make it possible to detect the slightest changes in the internal environment of the organism, its homeostasis. The existing laboratory and instrumental methods to diagnose diseases of the lungs are undergoing further improvement. Greater attention is given to identification of causative agents of inflammation (including the agents of the new generation, such as viruses, fungi, etc.). Comprehensive bacteriological studies with new elective nutrient media facilitate the correct diagnosis. Methods for rapid aetiologic diagnosis of pneumonia are being developed. Immunoassay techniques help reveal such causative agents as Chlamydia, Legionellae, or viruses.
The study of the immune status of the body has become a major item in revealing allergic pulmonary disorders. This includes detection of specific and non-specific antibodies, determining the immunoglobulin and immune response mediator levels, studying the structure and functional characteristics of immunologically competent cells using monoclonal antibodies, etc.
Methods of functional diagnosis of pulmonary diseases has been used on a wider scale too. Computers help better estimate the parameters of the external respiration. The flow-volume analysis makes it possible to determine the patency of large, medium, and small bronchi and this provides
for differentiated approach to the management of patients. Rheographic methods for determining the contractile function of the right ventricle, vascular resistance to the blood flow, and pressure in the pulmonary artery system are used in haemodynamic studies of pulmonary circulation.
Diseases of the pleural cavity, subpleural portions of the lungs, and the anterior mediastinum are more commonly diagnosed by ultrasonography. Thermography is more frequently used for rapid diagnosis of these conditions by detecting local changes in body temperature.
Roentgenotomography is now widely used for differential diagnosis of pulmonary diseases. Diseases of the lungs and the mediastinum, that are difficult to diagnose by common radiologic techniques, may be identified more reliably by computed tomography and scintigraphy. Radiocardiogra-phy and radiopulmonography are more frequently used for haemodynamic studies of the lesser circulation.
The diagnosis of various bronchopulmonary diseases is facilitated by endoscopy (fibrobronchoscopy, mediastinopleuroscopy) combined with biopsy of the bronchial mucosa and transthoracic needle biopsy of the lungs with subsequent cytologic, histologic, and bacteriologic studies of the obtained specimens. Percutaneous target biopsy of thoracic pathological formations is performed under the control of computed tomography or ultrasonography. The diagnosis of circulatory disorders is commonly made with employment of enzyme immunoassay methodologies to reveal atherosclerotic lesions of the blood vessels. High plasma lipoprotein levels are determined both quantitatively and qualitatively. The genetic councel-ling methods are commonly used to reveal a familial predisposition to atherosclerosis. Electrocardiography is commonly used for differential diagnosis of cardialgias and early diagnosis of ischaemic heart disease (pedalling tests with the determination of tolerance to exercise, and drug tests to correctly interpret changes in the ECG).
A new generation of computerized electrocardiographs have been introduced into clinical practice. Depending on the object of investigation, an automatic ECG analyzer is able to differentiate ECG changes in detail and give to 120 variants of conclusions. Computerized electrocardiographic systems have become an invaluable aid in regular medical population checkups. The ECG findings can also be deciphered in the form of simple conclusions, such as 'health', 'pathology', 'additional examination required', etc.
Day-round monitoring with stationary or portable apparatus is widely used to diagnose diseases of the heart. This provides important information on the character of cardiac arrhythmias and ischaemic disorders in the myocardium that develop in the patient in various situations (at rest or during exercise) during a 24-hour period. Cardiac monitoring reveals latent changes that cannot otherwise be detected during common short-duration electrocardiography.
41*
Appendix
Developments in Laboratory Diagnosis
Remote control of ECG is being further improved and special consultation centres are being established where ECG are deciphered in different cases. Computers are also used for integrated assessment of the course of myocardial infarction.
Rheographic methods of examination (bi- and tetrapolar rheography) are used to measure the main parameters of the central haemodynamics (stroke and minute volumes in particular). Using multifunctional polycardio-graphs enables electrocardiographic, phonocardiographic, and sphygmo-graphic examination to be performed simultaneously with rheography.
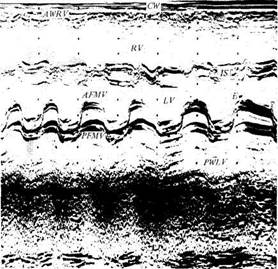
Ultrasonography is an effective means of diagnosis of cardiac pathology. It helps to verify the character and severity of pathological changes in the heart valves and in the myocardium (heart defects, dilatation of the heart chambers, contractile dysfunction), to reveal the changes in the inter-ventricular septum, dysfunction of the papillary muscles, prolapse of the mitral valve, postinfarction aneurysms, pericardial effusions, and new-growths (Fig. 113). Two-dimensional echocardiography helps accurate determination of the myocardial dysfunction and the volume of the heart
| INI |
llllllll
chambers. Doppler echocardiography, which is based on the changing frequency of the echoed signals, is also used for the examination of cardiac performance, determination of the effective stroke volume, regurgitation and shunting volumes, and the linear velocity of the blood flow in the arteries, and for detection of atherosclerotic lesions in large arteries and thrombosis of deep veins. Catheterization with subsequent ventriculography and biopsy of the myocardium is performed to reveal the cause of myocardial lesions.
New methods of studying blood vessels have been developed. A system for studying microcirculation during biomicroscopy of capillaries is provided with a special device by which the image is transmitted on the TV screen to supply comprehensive information about the condition of the microcir-culatory bed. Peripheral microcirculation (e.g. in the hands) is commonly estimated by thermography. Coronarography is used for special indications to verify the morphological changes in the coronary arteries in living subjects.

Fig. 113. Echocardiogram of the anterior flap of the mitral valve in mitral stenosis.
CW— chest wall; AWRV—anterior wall of the right ventricle; RV— right ventricle; IS—interventricular septum- LV—left ventricle; AFMV-anterior flap of the mitral valve; PFMV-posterior flap of the mitral valve; PWLV-posterior wall
of the left ventricle.
Fig. 114. Sonogram of a patient with cholelithiasis.
1—gall bladder cavity; 2—calculus; 3—acoustic path' (a characteristic sign).
Appendix
Developments in Laboratory Diagnosis
|
Noninvasive methods of examination of blood vessels (dynamic scinti-graphy, ultrasound examinations, computed tomography) are widely used.
|
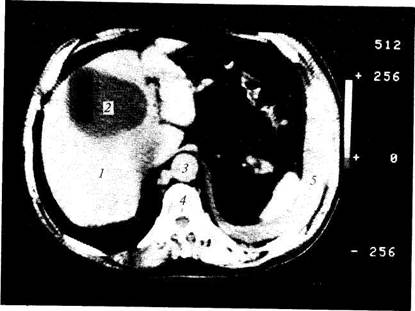
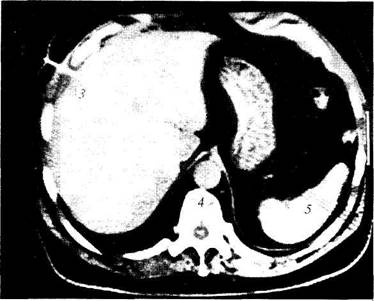
| Fig. 115. CT scan of hepatic tumour. 1—liver; 2—tumour node; 3—aorta; 4 —vertebra; 5—spleen; 6—intestinal loops. |
In gastroenterology, ultrasound is commonly used to diagnose diseases of the pancreas and liver, and also lesions of hollow organs such as the stomach and the colon (Fig. 114) (also combined with endoscopy). New-growths are detected by computed tomography (CT) and nuclear magnetic resonance (NMR). Computed tomography is a technique of diagnostic radiology that uses a narrow collimated X-ray beam, that is passed through the body (scanning), to produce an image of the studied tissue (organ) with the aid of the computer. This very precise technique makes it possible to differentiate between tissues with only slightly differing attenuation coefficients without using any contrast, and thus to detect pathological changes in them, e.g. hepatomegaly and tumour of the liver (Fig. 115), hydatid disease (ecchinococciasis) (Fig. 116), the gall bladder lesions (Fig. 117). Diagnostic percutaneous aspiration biopsy of a pathological focus may be performed under CT control to assess the cellular composition of a tumour (morphologic studies), to drain an abscess and introduce antibiotics into its cavity (Fig. 118), or to administer drugs inhibiting the malignant tissue growth into a tumorous node.
Fig. 116. CT scan of a patient with severe hydatid disease.
1—hydatid cyst in the right lobe of the liver; 2—daughter hydatids in the cyst's depths; 3—calcification line in the periphery of the cyst; 4—vertebra; 5—stomach.
Diagnostic radiology now includes large-frame fluorography of the stomach and percutaneous cholangiography. Angiography is more intensively used to reveal tumours of the gastrointestinal tract.
Endoscopy has also broadened the field of its application. TV endoscopy, endoscopy employing microelectronic devices, and luminescent endoscopy has been widely used in clinical practice. Endoscopic retrograde cholangiopancreatography is used to verify the condition and patency of the extrahepatic bile ducts. Inflammation of the internal organs is diagnosed thermographically (endoscopic thermography). Complex automated instruments employing microelectronic devices and also multichannel recorders of bioelectric processes in the gastrointestinal tract are being devised.
Histochemical, immunochemical, genetic, historadiographic, and electron microscopic techniques are widely used for the diagnosis of gastrointestinal pathology. The determination of concentration of gastrointestinal peptides in tissues, the activity of various enzymes in the pancreatic juice, and studies of upset digestion and absorption in the small intestine also help the diagnosis.
|
|
■! ■
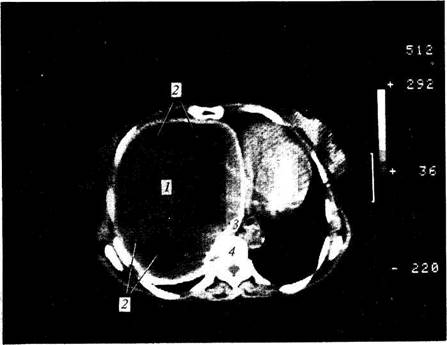
Fig. 117. CT scan of a patient with cholelithiasis.
1—enlarged gall bladder; 2—concretion of uneven density; 3—liver; 4—kidneys; 5—vertebra; 6—intestinal loops.
Developments in Laboratory Diagnosis
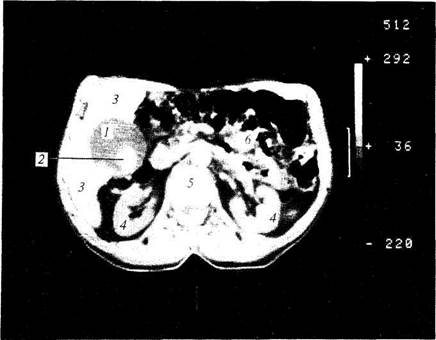
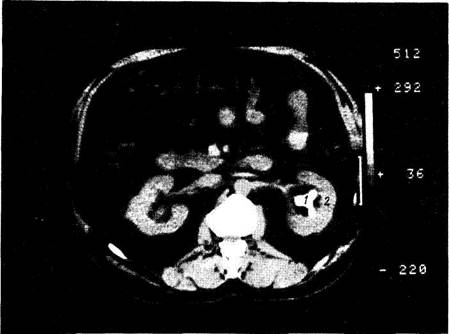
Clinical practice has been enriched by highly informative methods of studying the kidney performance. Immunologic diagnosis of various glomerulopathies and bacteriologic studies in pyelonephritis undergo further development. Ultrasound and radionuclides, computed tomography and selective angiography of the renal vessels are widely used in the diagnosis of nephrogenic arterial hypertension, tumours and cysts of the kidneys, and nephrolithiasis (Fig. 119). Nuclear magnetic resonance and tomography facilitate assessment of the kidney function by producing separate images of the cortex and medulla. The condition of the retroperitoneal space may also be better assessed.
| Fig. 119. CT scan of a patient with nephrolithiasis. 1—dense pathological formation with irregular outlines (calculus); 2—pelvis ofthe left kidney. |
Computed tomography is commonly used to diagnose endocrynological disorder, e.g. abnormalities of the adrenals (Fig. 120). Diseases of the thyroid (neoplasms, cysts) are well detected by echography which is also helpful in detecting enlargement of the adrenals.
Fig. 118. CT scan of puncture of liver abscess.
1—liver; 2—liver abscess; 3—puncture needle; 4—vertebra; 5—spleen.
Appendix
Developments in Laboratory Diagnosis


|
A correct diagnosis can be established only on the condition that the physician has adequate clinical thinking and is able to analyze and correlate the patient's complaints, history, and physical examination findings with numerous additional information obtained in the laboratory and by instrumental examination.
 Fig. 120. CT scan of a patient with tumour of the left adrenal gland.
Fig. 120. CT scan of a patient with tumour of the left adrenal gland.
1—tumorous masses with signs of calcification in front of the left kidney; 2—left kidney; 3—aorta; 4—normal right adrenal gland; 5—inferior vena cava.
Advances in the diagnosis of internal diseases in the forthcoming decades largely depend on the development of new diagnostic techniques based on recent scientific and technical progress, and on equipment of tus, the physician can sometimes underestimate the importance of subjective hospitals and policlinics with new apparatus and instruments. At the same time, such technization of medicine has some adverse effects. Being supported by accurate and highly sensitive laboratory instruments and appara-symptoms of the disease and the informative value of such techniques as palpation, percussion and auscultation. Meanwhile, each physician must be able, in case of emergency and in conditions where such instruments and apparatus are not available (e.g. at patient's bedside), to establish the diagnosis and render appropriate medical aid. The physician must not entirely depend on an X-ray apparatus or a laboratory; such a physician is then only a dispatcher who refers the patient to the laboratory for additional examination.
 Developments in Laboratory Diagnosis 629
Developments in Laboratory Diagnosis 629
Table 7 Residual Non-Protein Nitrogen and Bound Nitrogen in Blood Serum
 Substance
Substance
Quantity
 Normal Laboratory Findings
Normal Laboratory Findings